Impacted Teeth Canines
Did you appreciate the information?

Introduction

Canine shape and position (red arrow)
A canine is an important tooth of the dentition because it is placed strategically in the mouth. It makes the transition between the anterior teeth (central and lateral incisors) and the posterior teeth which are the first and second premolars. This tooth has a very long root, the longest of all teeth, and therefore, its position is unique in the dental arch.
• Function: It is a strong and solid tooth designed to tear foods. It is also used to guide the movements of the lower jaw during chewing.
• Esthetics: The color of the canine, generally darker, ensures the transition between the incisors which are often lighter in color and the posterior teeth. The sharp shape also plays a role in the transition of the visual esthetics between the anterior and posterior teeth.
• Eruption: It erupts after the premolars in the maxillary arch. Being the last one to arrive, it often has to put up with limited space. As it is a big sharp tooth, it is not uncommon to observe its prominence and its malposition. The canine usually erupts before the first premolar in the mandibular arch, but it sometimes happens that the order is reversed and, like its counterpart in the maxillary arch, it puts up with the remaining space.
Impaction and ectopic eruption
A canine is considered impacted if it does not come into the mouth and remains in the alveolar bone in an ectopic position. Ectopic means: “that is not at the right place”.
Impacted canine in vestibular position

Impacted canine in vestibular position
A canine can end up on the palatal side (palatal impaction), stay very high and horizontal above the other dental roots (see #2 on the picture and the X-ray of impacted canines) or be prominent in the oral vestibule (impaction on the vestibular position: see #1, #2 and #3 on the picture), that is on the opposite side of the palate.

X-ray of 3 impacted canines
We then talk about vestibular impaction, meaning that it is positioned in the oral vestibule compared to palatal impaction, where the canine is on the palatal side.
Palpating the areas identified by circles makes it possible to feel lumps revealing the presence of canines. Visual examination shows that the lateral incisors are very inclined. They are inclined because the canines represent an obstacle to the good positioning of the lateral incisors. The vestibular impactions represent only 15% of canine impactions.
Palatally impacted canine
In 85% of cases, canines are impacted on the palatal side. In the same way as previously, palpation and visual inspection make it possible to suspect the presence or the absence of such ectopia.

Palatally impacted canine and follicular cyst (group of arrows)
The circle on the picture on the opposite side represents the lump of the palatal vault that is easily palpable with the finger. A white arrow indicates the displacement on the palatal side of the lateral incisor crown, which means that the root is on the opposite side of the crown. It is thus called a vestibular root. It is like that because of the presence of the permanent canine that is just beside, on the palatal side. The persistence of the primary canine is also another visual indicator. On the X-ray, the group of white arrows defines the border of the follicular envelope that surrounds the tooth crown and it is much enlarged. At this size, the envelope is a follicular cyst and as with all cysts, it will tend to get bigger and wider, causing damages to the surrounding teeth (resorption of the root, movement of teeth or pathological evolution of the cyst).
Incidence and prevalence
Canine impactions involve 0.92% of the white American population. Epidemiological data shows different incidences among other populations.
• Finnish = 1.8 %
• Swedish = 1.7 %
• Italian = 2.4 %
• Japanese = 0.27 %
• White American = 0.92 %
Canine impactions are more frequent among females than males (F : M = 2.3 : 1) or 1.17% of females and 0.51% of males. And, as it was previously mentioned, 85% of impactions are palatal impactions compared to 15% that are vestibular impactions.
Etiology
Research shows that the cause of canine impactions is mainly hereditary, therefore genetic. Among other causes, there is persistence of the primary canine (the root does not resorb), an infectious chronic periapical lesion (at the apex (tip of the root) of the primary tooth), pathology issued from the follicular envelope such as dentigerous cyst or a giant cell tumor.
Proofs concerning the genetic origin of an impacted canine are the following:
• Link with other dental anomalies.
• Peg shape teeth or microteeth.
• Congenital absence of a lateral incisor.
• Infraocclusion or ankylosis of the 2nd primary molars.
• Congenital absence of one or both lower 2nd premolars.
• Delay in the formation or distal angulation of the lower 2nd premolar.
• Occurs bilaterally, that is on both sides.
• Dr Ann Todd convened a research among files of the Harvard University’s orthodontics department and she found that when a member of a family has an impacted canine, 40% of the members of this family (brothers and sisters, cousins, uncles and aunts) had an impacted canine.
• Sexual dimorphism. More females have impacted canines than males.
• Difference across populations.
Peck S, Peck L, Kataja M. The palatally displaced canine as a dental anomaly of genetic origin. Angle Orthod 1994;64:249-256.
Peck S, Peck L. Palatal displacement of canine is genetic and related to congenital absence of teeth. J Dent Res 1997;76:728-729.
Todd, A. , Cephalometric and epidemiological findings in families with PDC, Angle East meeting, Charleston, 2008
On this figure composed of 3 X-rays of 3 individuals of the same family (2 brothers and 1 sister), you can see, for the girl, the first signs of the impaction of an upper right canine as well as the enlarged follicular envelope and the congenital absence (hypodontia) of a lower incisor.

Impacted canine, family incidence and link with other anomalies related to eruption.
Her 2 brothers each shows an impacted canine and congenitally missing of both lower 2nd premolars. This is a single example among many more that I have come across.
Non-genetic etiology
Even though the genetic origin of impacted canines is confirmed, there are other factors that can cause the impaction or ectopic eruption of a canine.
Other causes can be:
• An infectious chronic lesion near the canine crown (chronic periapical lesion of a primary tooth)
• A dental or odontogenous tumor, a keratocyst, a giant cell tumor, a follicular or dentigerous cyst
• Impacted canine and chronic apical lesion:

Periapical lesion, pulpotomy and impacted canines
This series of X-rays shows well the problems that can create inflammation or infection to the apex (tip) of the root of a primary tooth (green “C” letter). The white arrows define enlarged follicular envelopes around the permanent canine crown (blue “C”).
The primary canines (green “C”) received a pulpotomy (partial removal of the pulp) because of a cavity or to reduce the sensitivity of the primary tooth when a cut is made through enamel and dentin. This results in chronic inflammation of the nerve and at the apex; this inflammation will be defined by an apical granuloma. This granuloma irritates the follicular envelope surrounding the permanent canine crown (blue “C” letter) and the granuloma becomes an obstacle in front of the permanent tooth. The tooth path of eruption is deflected. Therefore, a potential cause to the development of a follicular cyst would be chronic inflammation of the apical granuloma. (Becker, A., The orthodontic treatment of impacted teeth 2e ed.Thieme 2007, p.97 & 240.)
Consequently, if the lack of space in the incisor-canine area necessitates proximal reduction (cut in enamel and dentin) of the primary canine, it could be more recommended to proceed with the extraction of the primary tooth. If this were the case, it becomes another chapter of the concept of interception in orthodontics which will be developed later on. You can consult the seminars Interception en orthodontie and réduction proximale sélective. Crowding of a primary canine and a lateral incisor of 1.5 mm does not justify the proximal reduction of the primary canine.
Solution: The cases shown above all required, as initial procedure, the extraction of the primary canines. Back.
• Impacted canine and odontogenous tumor.

Giant cell tumor, impacted canine
This kind of pathology is not very frequent. It is the reason why when we encounter one, we remember it. It is an 11-year-old young girl who comes in for misaligned central and lateral incisors and for a palate that is too narrow (there is a crossbite on the left side). Visual examination shows a bulge of the cortical plate (black circle) and a different vascularization of the mucous membrane. The radiographic appearance of the cyst, apart from an enlargement that can be seen very easily, is similar to a benign lesion. The extraction of the primary canine was prescribed as it is always the case in such situation. In short, the bulge of the plate increased in the following weeks and taking a new X-ray showed the enlargement of the cyst. The patient was referred to oral surgery and in Dr Dany Morais’ expert hands, the cystic lesion was removed entirely and pathological examinations were performed. Back.
• Impacted canine and lack of space

Impacted canine and lack of space
Here is a typical example of an impacted canine (black circle) caused by a lack of space in the dental arch. In the current case, there is no space available between the 1st premolar and the lateral incisor to put a canine of 8 mm in width. Both sides are affected. Back.
Complications, consequences
An impacted canine, if it stays impacted, is a complication in itself.

Ectopic canines
It can also erupt late (whenever in adulthood) in a rather unusual area (ectopic). The case shown on the opposite side shows the retained primary canines (red arrows). Permanent canines finally erupted in the mouth despite the obstacles which are primary canines and the lack of space. The upper right canine (blue arrow, position 1) is on the palatal side. The upper left canine (blue arrow, position 2) has erupted in the oral vestibule in front of the lateral incisor. The lower left canine (blue arrow, position 3) has erupted on the lingual side.
In conclusion, keeping a primary canine in the mouth beyond the timeframe where it should normally shed guarantees that the permanent canine is either ectopic or impacted.

Impacted canine and radicular resorption
Another complication is the resorption (shortening) of the roots of the adjacent tooth. Note the resorption of the roots of lateral incisors. As a metaphor, it is as if the collision between the permanent canine and the incisor had pulverized the root.
Preventive diagnosis
The permanent canine normally erupts around 11-12 years of age. It is thus wise to verify its position and its evolution as early as 9-10 years of age. We must suspect that an anomaly can occur if we observe:
• A microtooth or a congenital absence of a lateral incisor
• An overall delay of eruption
• The retention of the primary canine beyond 12-13 years of age without any signs of moving
• A palpable palatal vault
• A congenital absence of premolar(s). One or more absent premolar.
• An ankylosis of a second primary molar
• A lateral incisor in labioversion, palatoversion, distoversion
Interceptive treatment
The extraction of the primary canine in relation with the permanent canine that shows an ectopic evolution is the treatment of choice of the interceptive measures to perform.
The decision is made from an early diagnosis, the patient is between 10 and 13 years old. The relative position of the permanent canine with regard to the adjacent teeth is an important factor in the success of the interception. By success, I mean that the canine will go back to a normal path of eruption.

Evaluation of chances of success in an autocorrection of the canine eruption
Erikson and Kurol developed a little evaluation diagram. If the tip of the unerupted canine does not go past more than half of the root of the lateral incisor (zone 2 and 3) and the inclination angle related to the medial plane is not greater than 55o, the average success rate (normal eruption) is about 80%. This means that 80% of the cases showed a normalization of the canine eruption in the 6 to 12 months following the extraction of the primary canine.

Success rate by auto-eruption
If the permanent canine is in zone 1-2, the success rate is about 90%. If the canine goes past the lateral incisor and the tip is in zone 4, the success rate decreases to 64%.
If no improvement is observed, then the autocorrection prognosis is weak and a procedure must be considered.
Ericson S, Kurol J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur J Orthod 1988;10:283-295.
Pitt S, Hamdan A, Rock P. A treatment difficulty index for unerupted maxillary canines. Eur J Orthod 2006;28:141-144.
Often, a path correction is observed and we can anticipate that the canine eruption will be normal. A second factor then steps in our decision-making process. It is time. Some canines can take up to 2 years before erupting in the mouth. After discussing with the patient, it can happen that the decision is made to proceed with the surgical ligation of the canine to make it erupt more quickly, not to delay the evolution of the orthodontic treatment underway.

Autocorrection of impacted canines
This example illustrates well how efficient the preventive extraction of primary canines (X) is to correct the path of eruption (white arrows) of permanent canines which deviated toward the palate and for which the vaults were palpable with the finger tip at the back of the lateral incisors. The X-ray on the right, taken 9 months after the extraction of primary teeth, shows favorable repositioning of the permanent canines. This case is among the several ones I was happy to manage successfully that way. Of course, in some cases, the repositioning was less spectacular and it was decided to proceed with an exposure surgery and ligation of the permanent tooth.
One thing is for sure, to not extract the primary canine guarantees that the permanent canine will remain impacted.
Pitt S and colleagues determined a treatment difficulty index for impacted canines. The important factors are:
• The horizontal position of the impacted tooth (degree of overlap with the lateral and central incisors).
• The patient’s age.
• The height or vertical position of the impacted tooth.
• The oro-palatal position of the impacted tooth.
Ericson S, Kurol J. Early treatment of palatally erupting maxillary canines by extraction of the primary canines. Eur J Orthod 1988;10:283-295.
Pitt S, Hamdan A, Rock P. A treatment difficulty index for unerupted maxillary canines. Eur. J Orthod 2006;28:141-144
Hi. I do not know if you still respond to these comments but I hope to hear from you.
My son is 8 years old and he has very crowded teeth and has a little bit of overbite.
I talked with 2 orthodontists and they have different opinions.
One of them suggested expanders for upper and lower jaw if I did not the extraction of adult teeth later. He did not mention anything about the extraction. I am concerned if extraction itself is enough and the expanders can wait or unnecessary. His lower jaw is receding in my opinion and do you think the expanders will help his lower jaw grow?
The other doctor recommended to extract 4 of baby canines asap to prevent impacted teeth, come back in 10 months and take CBCT. I am afraid if it will be too late after we wait 10 months and he will have no space for permanent canines(I was told there will be no space maintainer) because I think once baby canines are extracted crowded front teeth will take their place to align themselves.
Which plan do you think is better?
Is it ok if I send his x-ray to orthochamberland@videotron.ca
Thank you
I am skeptical. At 8 years old, it might be to young to diagnose impacted canine,but not too young to diagnose lack of space and recommend serial extraction.
If ther is lack of space enough then extraction can be indicated. Later, extraction of the 1st primary molar can be indicated follwed by extraction of permanent premolars.
I don’t know what would be best for your son, becaus I did not see him. Yes you can send the panogram at the above email.
Dear Dr. Chamberland,
Our 12-year old daughter does also have two impacted upper canines.
One of them is going to be extracted.
I’ve sent you some x-rays to drsylchamberland@videotron.ca
It would be very nice if you could have a brief look at it!
Thanks in advance.
Best regards,
T. Kuhn
I might be too late to reply, but why extract one canine and nont the other. What will happen if only one permanent tooth is extracted?
Hello Doctor,
I truly appreciate all of your responses to the previous commentators. Anyhow, I am 21 years old and I have an impacted canine on the left side of my mouth and it is completely horizontal and possibly fused to the roof of my mouth. I don’t have photos at this current moment. Bringing the tooth down via chain and braces method is a long shot according to the orthodontist. My issue is with the impacted extraction surgery itself, what are the surgical risks? Is it possible to remove the canine and keep the baby canine tooth?
It is the role of the surgeon to explain you the risk of the extraction. My concern is that the primary teeth may not remain stable troughtou your life. At 21 years old, the prognosis of bringing this impacted canine into occlision is usually very good altough it may take 1-2 years.
I am 13 years old and my orthodontist said that because of the fact that he couldn’t bring my permanent canine down he would give me two options. The first was to get the permanent canine removed along with the milk tooth, have a false tooth and use braces to straighten the teeth. The second was to remove the permanent canine and the milk tooth along with some molars and use braces to straighten the teeth. I have minor crowding in my lower jaw and severe crowding in my upper jaw because as a result of my impacted canine one of my incisors has grown in my palette instead. If you could not bring the canine down would this be the course of action you would take?
There may be an indication to extract permanent teeth. It could be the impacted canines, but it could be the 1st premolars. But you definitely need braces. I do not recommend a false tooth.
Dear L,
You need to comprehend that the teeth that shifted toward the missing canine have to be recentered. Therefore you will likely need comprehensive orthodontic treatment. This may include extraction of premolars if there is not enough space.
However, it is possible that you don’t need extraction. I can’t tell because I don’t have enough information.
If you choose to extraction the impacted canine only and get space close, the teeth deviation may only get worse.
Claudia, yes it will help because I am getting confuse. The flow of answer does not indent orderly and it get me lost to whom am I answering.
There is a possibility that the roots of the incisors already have some damange.
There is a possibility an orthodontic traction of an impacted canine could damage the root of the incisors, but the direction of traction is very important as one should pull the canine away from the roots from start.
I don’t know your age, but I usually try to bring the canine although there are some circumstance I will decide or have to extract the impacted canine.
I apologies for not uploading an exemple. It seems that there is a blocage in the system.
There is a possibility that the roots of the incisors already have some damange.
There is a possibility an orthodontic traction of an impacted canine could damage the root of the incisors, but the direction of traction is very important as one should pull the canine away from the roots from start.
I don’t know your age, but I usually try to bring the canine although there are some circumstance I will decide or have to extract the impacted canine.
I apologies for not uploading an exemple. It seems that there is a blocage in the system.
Hello doctor Chamberland,
Thank you for your help! I don’t know which type of crossbite I have. I’ll send a picture of my teeth at your e-mail address, if it is ok.
Thanks for sending the photo. You have a cross bite of your upper right lateral incisor with the lower right canine. I understand that the radiography that you sent me was flip horizontally. I thought it was your left maxillary canine, but in reality, it is the right maxillary canine.
From the pircture I saw, it seems that the crossbite extend to the 1st and 2nd upper right premolar. If true, how will it be manage?
I agree that the lateral incisors should not be bonded nor engage into the main archwire until the palatally impacted canine is not displaced. Will you have a surgical exposure and orthodontic ligature of the canine?
I have been told that I have an impacted canine tooth (upper right) and that they had to remove the tooth otherwise it could damage the roots of the other teeth it has grown nearly completely horizontal and they said that it will be near on impossible to move it into its proper position without damaging the roots of other teeth what should I do?
Ask him how he plan to correct the posterior crossbite?
Each ortho may have his own plan, but I would first extract the primary canine, ask for surgical ligature and begin the orthodontic traction.
If you have posterior crossbite, then it should be plan to expand the maxilla. This is can be done at the same time with proper appliance. The new Maxillary Skeletal Expander (MSE) would work for you. I comprehend that you can do the canine traction followed by the maxillary expansion.
Keep in mind that you mention in your first post “lateral crosbite”, which I interpret as a posterior crossbite. I may be wrong. You may meant crossbite of the lateral incisor.
Can you confirm wich type of crossbite you have?
I would NOT extract the permanent canine.
Hi,
I am 28 and have a top impacted canine, which has not affected me since acknowledging this. When I was around 16, I had terrible tooth pain, infection and the baby tooth was extracted, and nothing was done about the impacted canine. It was therefore left with the xtracted space gap. This gap has now gone smaller (although still there and bothering me) but the front tooth near it has also shifted and started to move a little into filling the space.
I wanted to close this gap asap- I had seeked orthodontic advice and was told invisalign or fixed braces wouldn’t be the best way forward, but to bring the impacted canine down? I am worried how this would work as there isn’t enough space for this and I don’t want to extract healthy teeth nearby? Ideally I wanted to extract the impacted canine and close the gap- either with braces/implant or dental bridge. What would be your advice on this?
Hello Dr Chamberland,
My almost 11 year old son has a horizontally impacted canine in his upper jawline. So far, we have been to see 2 specialists, neither of which have given us a clear approach to the issue. One suggests removing the baby canine tooth and removing the impacted one so that the space is reserved for an eventual implant, while the other suggests removing the baby tooth and leaving the impacted tooth in place. As well, my son seems to have a conical shaped incissor on the same side, but it is unclear as it is still coming in and is inwards in his palate. I was wondering if I might be able to send you a picture of the panoramic xray to have an opinion on the best course of action.
Thanking you in advance for any suggestion you may have for us.
I agree to remove the primary canine, but NOT the permanent canine. Forget an implant for such a young person.
Send the xray to orthochamberland@videotron.ca
Hello dr. Chamberlaid,
I’m 34 years old and I have an impacted canine (13) and lateral crossbite. The crown of the impacted canine is very low, just above the central incisor. I’d like to send you my panoramic but not sure how to do it (I don’t have facebook). I visited 2 othodontics, one said to remove the milk tooth and try traction of the canine while the other advised removal of impacted canine and an implant. What is your opinion, what should I do? Thanks
My 13 year old daughter (will be 14 in March) had a panoramic taken at her recent check-up. She has her adult lower canines, but her upper canines are her baby teeth. The panoramic shows her adult upper canines and their positions. Though the dentist said one of the adult canines is in good position, if she pulled the baby tooth on that side there would be a huge gap and she wasn’t sure if that was the right approach; my daughter has a lot of space there, as if the adult canine is pushing the baby tooth to the side.
On the other side, the adult canine is tilted in the wrong direction. Both baby canines still have root retained and neither are wiggly. If the baby tooth beneath the crooked adult tooth were pulled, do you think there is a chance the adult tooth would straighten toward the gap on its own, or is this a definite case for orthodontic intervention?
I have never been to an orthodontist before for any of my children and just want to avoid over-treatment. My daughter has no discomfort with her gums, teeth or bite. It seems one side might just have the baby tooth pulled and the adult tooth is ready to descend, but the crooked side concerns me.
I have been reading your site and everyone’s cases and questions, and would appreciate getting your thoughts on my daughter’s canines, so I can be more knowledgeable about what may be needed, what approach/es would be most reasonable, and what may not be necessary. Merci beaucoup.
I don’t have Facebook, so here are links to a dropbox for your review:
panoramic: https://postimg.cc/sMwYNVHq
tooth spacing, 3 pics: https://postimg.cc/gallery/1fagq2c9g/
Without any hesitation, you should extract both primary canines (marked with X). The upper right canine will erupt soon in the space. The left canine will need surgical exposure and orthodontic traction.
The gap created in the mean time is a minor issue that will be solved by the orthodontic treatment.
Doctor, thank you so much for this reply and your observations on my daughter’s retained upper canines. We will seek orthodontic care directly after the holidays.
Looking at the diagram in your “Interceptive Treatment” section on this page, I am guessing that her upper left canine position is at least zone 4 or beyond, and thus needing the orthodontic corrections you recommended.
I have seen both open and closed exposure methods discussed online. Are exposure methods are different depending on the location of the impacted tooth (either in front of or behind its correct position)?
I do have one other child with a similar issue (retained upper canines). Two of my children (twins) had no issues with shedding all baby teeth and the positioning of adult teeth, and two have this retained canine issue.
Her images:
https://postimg.cc/wy97kGwv
https://postimg.cc/d734W5Dq
One upper baby canine (the right, I believe) was being pushed outward by the adult tooth like a “fang” sticking out of place, and once it was extracted, the adult canine slid into position without trouble. The adult tooth had already broken through the tissue and was wedged behind the stubborn baby tooth. This panoramic was taken prior to that extraction. The photo of her teeth is current, showing one adult upper canine and one remaining baby canine.
We have not had the opposite baby canine removed yet, (she is fearful of extractions and dental treatments) but I really want this to be resolved for her, so there are no more worries (and no more baby teeth).
I am wondering if the position of her left upper adult canine looks good so that extraction of the remaining baby tooth would allow it to come into position on its own. If so, perhaps we can avoid an orthodontist in this case (no offense intended!) 🙂
Merci, et bonne année 2020!
Claire
I found out that I did not answer your question. The answer is Yes, you should remove the primary canine.
Hi,
I am 30 years old women, i have impacted upper canine, because of that i have gaps and i want to close the gaps.when i first visit my orthodontists he requested to see 3D image of the canine and he said he will not be able to pull the canine down because one is close to my nostrils and the other one on my left side might damage the roots of central and lateral incisor. but after looking at 3D image he said they are palatal and recommended to put brace on to close the gap by substituting the first premolar in place of canine and the impacted canines will be removed anytime after the gaps are closed or just leave as impacted. Now 7 months after straightening all teeth he is asking me to choose between extracting the impacted canine before closing the gap or just closing the gaps with taking 20% risk of root shortening due to the impacted canine. i am really worried what to choose.i don’t have any courage to extract the canine because it is close to my nostrils and sinus. i can attach you my x-ray picture but i don’t see any option for attachment.
thanks,
The faith of the canine should have been decide before initiating the orthodontic treatment. The fact that the canine was high doe not mean it is not possible to bring it into occlusion. However, there was a risk that it could be ankyloses or become ankylose during treatment.
At this stage, I can’t recommend to change the treatment plan, therefore, you should procedd to extract the impacted canine and then close the space. I WOULD NOT try to close the space if the canine are still impacted.
I was told today that my daughter wouldn’t have wisdom teeth. How does the dentist know?
He probaly took a panoramic xray and there was no tooth buds of the wisdom teeth.
Hello! I just got my braces on three days ago because I have an impacted canine .. my baby canine is going to be extracted next Tuesday and then I hope the permanent canine will come down by itself.. I am 15 years old and I was wondering what you think how long that process might take?
Is there a chance I could send you the x ray where you can see my impacted canine?
It may come by itself but it may take 6 to 12 months. You can send the panogram via my professional facebook page.
Hi Dr. Chamberland!
I am a 23 year old with a platally impacted canine. I still have the retained primary canine. The retained primary tooth has slowly began to decay over the past 5 years and it now has a noticeable cavity that has formed on the side of the tooth that meets the neighboring molar. It is not causing me any pain or discomfort the only complications are the embarassing aesthetics of it (noticeable black spot and size). My other issue is the upper canine on the adjacent side DID erupt as a child but it is causing me to have a severe cross bite and unpleasant smile since it is basically “caved inward” towards the roof of the mouth which causes it to rest behind my lower canine when I bite. And lastly, my two upper front teeth seemed to have suddenly shifted tightly together causing me pain and pressure and making it hard to floss. So My questions are
Since I can’t afford the typical surgery it would take to correct my issues can I start by correcting my cross bite with invisalign? And then have a crown placed on the retained primary canine to meet aesthetics? And what could be causing this sudden tight shift in my front two teeth, could it have anything to do with the impacted canine or possibly root resorption? Thank you for any advice you can offer me! I can also send you photos if needed.
The retained primary canine will not survive to cerammic crown. You will loose both the canine and your money.
Your case is very comlex and is not fitted for Aligner therapy.
The best treatment you can have is full comprenhensive treatment with braces and traction of the impacted canine.
You can send photo via my professional FB page.
Hi Doctor,
Thank you for your valuable response, I sent the X-ray, pictures and the picture of that bite corrector by email. Because my son also has a little bit cross bite, the corrector will fix it also for making space for canine come down. Actually I don’t want the way to extract the teeth. I’m just wondering is there the way to fix the problem without extracting the teeth. Thank you for your time!
Best regards
Yang
I don’t recal having received the X-Ray of your son. Of course, if there is a cross bite, a rapid maxillary expansion is indicated and the need for space (or extraction) should be reassess after RPE. Often time, after expansion, there is enough space.
Hi, my 11 years old son has his upper permanent canine tooth come out from his gum, and his upper front two teeth kind of shift to one side. We went to the two orthodontist and they give different ways to let let the canine tooth come to the right place, one is extract 4teeth and put braces. Another is to put:
1. Bite corrector appliance (for about 6-8 months)
2. Invisalign (for about 12-14 months)
3. Retainers after treatment
I don’t know which is the perfect and suitable plan for my son’ s case, for us we don’t want to extract teeth, so if possible would you please give us some advice and the way to fix my Son’s canine tooth, thank you very much!
Can I send you the X-ray by email, because I don’t have Facebook
I don’t think Invisaling would be effective to treat impacted canines.
If the front teeth are shift to one side, this mean that there is space loss on that side and the canine will be ectopic. Extraction of 4 teeth is not a bad treatment plan.
I don’t know what you mean by a “bite corrector appliace” There is so many appliance. This name is to vague.
You may upload xray to a dropbox and send me the link in the comments box of my website.
Hello, my daugher is 12 years old. I was told that “13-23 are buccaly placed without space to form maxillary arch”. This was just after a visually exam,there is some space but I am wondering if should we wait a little and see if they nicely completely erupt or start to contact and orthodontist.
If the canine are place buccally and between the roots of the lateral and the premolars, you could wait and reassess in 6 months. If the canine are place buccally over the root of the latera incisors, you should not wait.
Don’t expect that the canines will align nicely if there is a lack of space.
I am 27 years old ad have an impacted upper canine. I can send an xray but not sure where. Do you think it is worth replacing the canine with the baby tooth and if not what other options do I have if the baby tooth decides to come off. thank you!
At t27 years, the best treatment is to remove the primary canine and bring the impacted canine into occlusion. You can not rely on a baby tooth long term.
I am age 59 with canine tooth still in the roof of my mouth. The primary is long gone, there is no space for it to move down. Any reason for me to have it removed?
There could be many reason to remove your impacted canine, but there might be some to just follow up each year. I can not tell without an xray.
Hi, My 8 & 1/2 year old daughter was referred by her dentist to an ortho because of her upper canines coming in crowded. I took her for 2 ortho consults. One ortho said do a rapid palate extender and front braces to make room for the canines and not damage the roots on the front teeth. The other ortho said to do nothing and wait and see if they come in normally. Do you think they’re in zone 1 or 2 and will come in normaly? Or should we do the RPE? I’ll send the X-ray to your Facebook. Thanks!!
Thank you for sending the panogramm to facebook.com/drsylvainchamberland.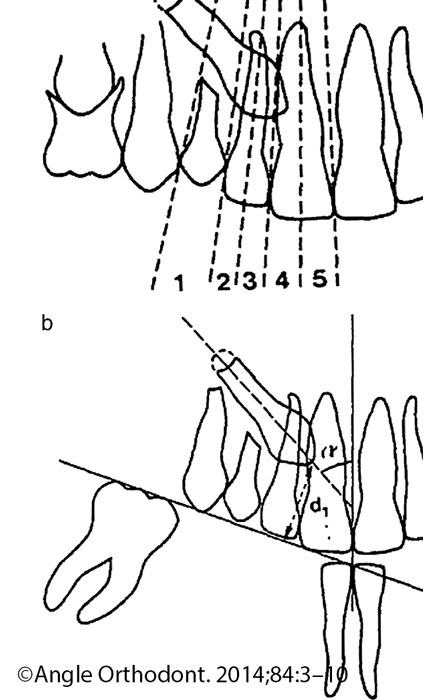
I would not worry at this age for the canine. They appear to have a favorable path of eruption.
They definitively not in zone 2. I would say it is in zone 1, which is a safe zone.
I would reassess in 1 year. If there is no posterior crossbite, I would delay palatal expansion.
Does-it answer to your question?
Hi Doctor.
I have an ectopic canine from the upper left side and had my braces recently but I just remove last 1 month ago.they exchange position from my lateral incisor but the problem when my doctor move to its original position the roots of my canine can’t move because of the lateral incisor. When I get second opinion to other orthodontist, and have my 3D xray. Then he see that I am having a bone loss from the canine teeth and should be stop on making a movements so that it will not worsen the situation. Now, his plan A. TO extract my canine and move my lateral incisor to its original position and had my dental implant/ partial denture on my canine after the braces treatment. Plan B. Is to interchange or my canine will be place to the lateral incisor and lateral incisor to canine but he told me that if he will do that there’s still possibility that I will lose my canine its because of the bone loss.
and just recently doc, I’ve notice that I have crack in my canine teeth.
I want to send my panoramic and
3D xray but I dont know how.
I want your opinion in my complicated case Doctor. Thank you
I also told you that removeing the canine or the lateral to place an implant is the worse thing to do. It will never be esthetic.
Moreover, if an implant is planned to replace the lateral, you are still stuck with the root of the canine in the way of the implants.
My best recommendation would be to find an orthodontist who know biomechanics.
Best regards
I am 34 with 2 impacted canines. In my 20s the ortho suggested I leave them impacted and close up the space. I wore braces for about a year and the space was not fulling closed. Now my teeth that belong next to the canines are shifting, since they dont have any support. Since the space is so small, I wonder if its worth trying to get the canines exposed. Would love to upload a panoramic.
Send your panoramic to my professional facebook account drsylvainchamberland
I’m 12 years old and I’m wondering if it’s normal to still have my upper canine teeth?
It may be normal at 12, but I would recommend that you visit an orthodontist and get a panoramic xray to assess the position of your permanent canines.
Hello Dr Sylvain Chamberland
Am 23 years old and I still have my milk tooth which wasn’t replaced by the canine tooth when I was little . I have been having a swell over my milk tooth for some good months now. When I went to the dentist he told me I should extract the milk tooth and see if my canine tooth is the one in the swell or not, I was afraid of staying with a gap so I didn’t remove it.
After reading your content, I have realised I can remove it since the real canine may errupt out. My milk tooth feels weak sometimes and when i over press the swell I feel little pain in my gum.
Should I remove my milk tooth out?
If I do so will my canine tooth come out from the swell?
Thank you so much.
You should get your milk tooth removed and have an orthodotnic treatment to bring your impacted canine in. You are only 23 and your permanent canine will last for your life.
I still have both of my child canine teeth, and my adult canines sit above them but protrude from the gums, is there any way this can be fixed? Is it advised to remove the baby teeth and hope they move into place or remove the adult teeth and hope the baby teeth don’t fall out? I’m 18 and I hate the way it looks to smile, I don’t think I can live my life looking like this for much longer
You are only 18. Remove the primary teeth and get an orthodontic treatment to bring your permanent canine in.
My daughters first tooth came only when she was 2 1/2 years old. Now she is 14 and her right canine has not come yet. She had the habit of thumb sucking and so the front teeth are very much protruded out. We showed the case to many doctors so that she could get braces.All the doctors are of the opinion that braces could be put only after the canine is out. Is there a chance that her canine might be impacted.Appreciate your opinion.
Thanks
Chances are that her canine is impacted and the at primary canine is retained. She may need surgical exposure and orthodontic traction.
I want to get your opinion on a very complex case of my 9 yrd old kid. I have got two mixed consolations from local Orthodontists. Since my kid’s case is very complex wondering if I can share her panoramic xray with you and get your opinion.
Findings:
A. She has midline discrepancy on the top
B. Narrow dental arches(top)
C. Impacted first molars #3,#14and slow eruption
D. Impacted Canines #6,#11 one is at an angle and other is close to nasal area sitting horizontally
E. Missing permanent lateral incisor #7
F. Slight open bite
G. Crowded teeth
Interceptive extraction of deciduous canine on palatally displaced maxillary canines
Bonjour Neha K and thank you for sending me the panogram. The best interceptive approach is to extract both deciduous maxillary canines (both marked X) and reassess in 6 months with a new panogram then 6 more months.
The best interceptive approach is to extract both deciduous maxillary canines (both marked X) and reassess in 6 months with a new panogram then 6 more months.
I agree that rapid maxillary expansion can help. I often do both. I mean expansion and extraction of the primary canines.Chances are that I would do it for you child.
However, it is useless at this stage to put braces on the central incisors unless there is a significant esthetic and social issues caused by dental spacing. You have plenty of time ahead to do braces that will be unavoidable anyway.
Regarding the prognosis of UR3 (#23 in FDI, #11 in your system), it may need to be expose and need an orthodontic traction. But you have plenty of time ahead to see what happen with interceptive procedure.
For sure she will need phase 2 comprehensive orthodontic treatment, but let her grow in the meantime (after exo of Cs and RME).
It might be to early to decide if we plan a dental impant at 18 or substitution of the missing teeth. Both option might be good.
I hope that help.
Our 15 year old son’s #6 upper right canine is impacted. The orthodontist has recommended braces for a couple months before having the primary canine removed while exposing and bracketing the permanent canine for pulling it down. In reading your article, which notes the evaluation by Erikson and Kurol, my son’s canine does not exceed 55% and it appears to be within zone 1-2.
Before having the above procedure done, would it be impractical to first consider having the primary canine removed and allowing time for the permanent canine to go back to a normal path of eruption?
(I do have a panoramic xray, but was unsure how to attach).
I would do extraction of the primary canine first, put braces soon after align the teeth and reassess 6 month later for the position of the canine. If it improve, one may decide to wait another 6 months or to do a surgery to epxose and attach it.
Thank you for your response.
My lower arch does permit. I am consulting with an orthodontist. I am on fast braces for almost a year and my teeth are worsening.
I just don’t understand why my orthodontist says he can’t move my canine as it will solve the problem.
I’m stressed as a small crooked canine straightened forward. He is straightening so my teeth r coming forward. I’m very unhappy.
My next visit is in 2 weeks. He booked a 45 minutes appointment. He says not to worry but I can c no improvement.
What do I do I have already made full payment.
Fast Braces is the new name of a bracket systems that was a comercial failes somes 20 years ago. In that time, it was called Viazis braces.
I can’t explain qhy the aligment of your teeth are worsening. May be you should get a 2nd opinion.
Fast braces DOES NOT mean “better.”
I am 40 yrs. My canine moved after 20 yrs of braces. My dentist fixed it. Now it crowded my front tooth and there is no space for my front tooth to move into place. There is space for the canine to move back. However my dentist says the canine cannot be moved back. Pls suggest an opinion to straighten my front tooth as one is not going into its place. Cam my canine go back just 2 mm
Your canine can move back if there is space behind and if the occlusion with the lower arch permits.
I recommend that you visit an orthodontist.
My 13 year old daughter has an impacted canine on her upper left side. She had both primary canines removed in Dec 2016. Since then the upper right canine has appeared, but the other left hasn’t.
One orthodontist recommends an incision on the gums and placement of a myo-trainer, and later use of orthodontics to correct an overbite, alignment of teeth, etc, saying that the root of the canine shows that it is in its final maturation stage.
Another orthodontist recommends beginning with Invisalign orthodontic treatment to move the teeth to allow the teeth to move out of the way, and that eruption of the canine is not age dependent.
I am unable to attach an image, but the canine is in the correct location, at an angle of 10-15%, and simply does not have enough space to erupt.
I am concerned that orthodontics may not be sufficient to allow the tooth to erupt.
Welcome your thoughts.
Myo-trainer is useless. It is fake orthodontics with no science.
It is not only the angulation that is important, but also the location. Is it palpable buccally or palatally.
It is true that making room will help the canine to self erupt. I would not use Invisalign if the canine is impacted, but Aligner therapy can move erupted teeth and open space for the missing canine.
You can send an image to my facebook.com/drsylvainchamberland
I will reply in this webpage.
I’m 24 years old & I have a impacted “eye tooth” it doesn’t bother me (no pain). I have noticed my gap that I have had is getting a little smaller. My dentist said in most cases that tooth will just stay put. Of course I don’t have thousands of dollars to under go surgery & when I was little the dentist again told me to not worry about it. I got my wisdom teeth out in May 2015 and tell gave me suggestions just in case I didn’t want the gap but didn’t seem concerned. Should I not worry about this?
An impacted canine may cause damage to the roots of the incisors. A cyst may develop around its crown. I wish you will consider an orthodontic tratment when you will have a more secure financial position.
Hello! I am 32years old and both of my canines are high and impacted. How likely will they both come down? So far, it’s been 4 1/2 months of activating the chains. I have xrays to show you. I will post to your professional facebook page. Thank you.
I don’t recall that you sent the panogram, but it may take 12 months, may be more to bring high impacted canine.
My 12 yr old son has a very horizontal impacted canine just above and between his two front teeth. The ortho said there’s no more hope to move it back because it will damage the 2 front teeth. She said it needs to be extracted and an implant done later. Is there really no hope? Could I possibly send you the pic so you can assess better? Thanks so much for your time.
I don’t know if it is too late, but you can send the pcit and xray to my professional facebook page or upload to a site and write the link here.
I would be very hesitant to recommend extraction of a permanent canie, but yes, in some case, it is a very good option.
My 12 yr old son has a very horizontal canine in his upper gums which is just above and between his two front teeth. Is there still any hope to bring it down to it’s rightful place or is extraction the only option? Looking at the xray pic, it seems like a very complicated case. Could you please tell me if there’s a chance to correct it and how the ortho and oral surgeon would most likely do? I can’t seem to wait for the orthodontist appointment which is not till mid Aug. and since I found out this week, I have been extremely worried everyday and feel so bad for my son. Could I send you a pic so you can assess better? Don’t know where I should send it to. Hope to hear your professional opinion. Thanks so much for your time.
Sorry for the delay. I am catching up for old comments and question. Your questions came when I was in vacations and it went burried under the pile.
The prognosis of bringing an impacted canine on a 12 years old boy is usually very good.
If you still need an opinion, you can post to facebook.com/drsylvainchamberland
I was surprised when the pediatric dentist asked us to see an orthodontist for my 9 year old child (never had dental issues, all very good exams for many years) because of TWO “impacting canines” on top.
The orthodontist though said that we need to have ALL FOUR baby canines PULLED as soon as possible and expensive SPACE maintainers ($1800) placed for the BOTTOM teeth after they are pulled (bottom teeth would crowd together and not leave room for canines to come out….top row would be fine without any space maintainers).
Theoretically, doing it this early…space opened up by extracting baby teeth will then (somehow???) persuade adult canines to MOVE automatically into place (without mechanics necessary now to pull top or bottom adult canines into position, chains/levers etc.)
Have you seen that in your practice?
The orthodontist would not give any percentages…like what is the percentage of chance this would actually work if we have baby teeth pulled immediately, versus waiting 1-2 years to see if they come out naturally on their own.
After all this is a bit of trauma for a 9 year old to go through…from NEVER having ANY dental procedures in her life to suddenly needing shots in the mouth, blood seen after pulling teeth, swelling afterwards, days of healing (not being able to chew easily etc.) and risking possible complications/infections…going from never having a fear of dental visits to possibly being scared.
Of course, we would like to do anything now that we have to do to avoid any future surgery requiring cutting gum or bone…or worse, pulling permanent teeth/having implants etc.
Also, orthodontist said the next panoramic x-ray would be at age 11 for my daughter, that it would be too much radiation to do it before then…but that it’s OK we won’t see for 2 years if extractions are successful, since teeth move very slowly.
And that she may require braces to fix canines between age 11-13 (costs like $10,000 here in my city in the U.S.!!! no one in my family has ever afforded braces and our teeth, we’re told, look great), since there’s no guarantee pulling 4 baby teeth now will fix alignment.
If you look at the panoramic x-ray, could you please give me a second opinion.
I do NOT have a Facebook account, but I would be more than happy to send you the panoramic x-ray via email if you email me from any account that you or your staff uses or if you direct me to a web page on your site that allows uploading of an image (since this form doesn’t seem to have that option).
Thanks so much!
At what age a canine may be considered impacted
This xray show a normal development of her dentition. Yes, you read well. I said NORMAL.
The 2nd thing I see is that she has spacing between her upper and lower incisors. Therefore she is not missing space that would justify extraction of the primary canine to help to align her front teeth. She has extra space. Extracting the primary canine will make it worse and increase the spacing between each teeth.
I would reassess the developement of her dentition with a new panogram taken in 18-24 months. She will then have 11 and if canine show signs of impaction, it will still be time to intervene. In my opinion, chaces are that the canine will erupt normally.
I would like to show you a similar case of a 9 years old girl who seek treatment for her protruded incisors and spacing.
I admit that the dental age is different bewteen the 2 girls, likeley 1 or 2 years. Your daugther barely have root formation of her lower 2nd premolar while my patient may have near half of the roots of the 2nd premolars that are formed. This explain why in 10 months, we see that the canine has moved favorably.
This means that we should wait before any intervention. Being patient is the key.
I hope that help.
Best regards
Dr Sylvain Chamberland
Your response helped tremendously, doctor!
I can’t thank you enough for your voluntary service… posting x-rays and suggestions on this web site (and doing it in your own limited free time).
Helping to inform the public…not just patients (and for children, their concerned parents) but also for less experienced orthodontists to learn more information about the movement of canines.
Thanks again!
The orthodontist, who seemed to have about a decade of experience (perhaps mostly with teens and adults), told this 9 year old girl in order to have a beautiful smile you need perfectly aligned teeth and perfectly spaced teeth.
She said to my child I want to help you achieve this beautiful smile…
So, I’m telling your mom you have impacting canines and an overbite which will make a smile not beautiful.
This caused my daughter to look in the mirror at home for the first time ever and ask me why her smile is not beautiful.
I am a mother, so I am subjective of course…but I think my daughter is gorgeous inside and out…and I told her some people in the world don’t embrace imperfections as being beautiful…especially in America where they spend a fortune to look unnatural.
I think it is not decent to tell a child her smile is not beautiful (especially when strangers we meet tell her how beautiful her teeth are)…her teeth are still coming in, she just turned 9 this spring…so there will be awkward stages…&
they are shifting and she has a growing jaw as well, so I am sure it is not perfect to any orthodontist…but we only came to her office because the dentist was worried the TOP permanent canines may be impacting the roots of the other permanent teeth and may not erupt properly, not for a beauty lecture.
I like how you phrase it on your web site if YOU do NOT like your smile, this is what can be done…rather than telling a young patient their smile is not beautiful and making her focus on something slightly imperfect that she didn’t even notice before this exam…and was 100% confident in every aspect of herself (her appearance, talents etc.)
Thank you again!
I am really thankful for tour reply.
We are not sure at what stage took place the resorption. I am afraid it happened at starting ortodontics 3 years ago. We just realized after one year of ortodontic treatment when they were about to fenstrate. They did not do a CT before starting.
Yes, I think they did use a cantilever spring now but after 8 months after fenestration it seems that nothing happens and it was pulling so strong on the front teeth that they do not want to make more pressure on them. The front teeth are suffering to much and they are really weak.
Now we have a new proposal from a 3rd orthodontist to use a kind of “micro screws” and try to pull the canines into the palate to separate them from the roots.
We are really lost with the whole treatment. We have tried two different doctors and no success at all.
I enclose pictures of 2015, study afrer one year treatment, when they realized resorption, new radioagraphy of April 2017 and a sample of the new proposal
I appreciate your kind information and your knowledge. Thak you
You told me that there was a 1st orthodontist who realised the resoption and the 2d who pulled during 8 months without success. You told me the name of the 3rd orthodontist you are visiting. He know how to use cantilever and miniscrew. I am quite sure that he can success to move the canine away from the root of the incisors and avoid further damage.
I would trust the 3rd orthodontist. I think he ca do the job. Keep me informed and would published the mechanics he use for your daughter and his name in my website if he accept.
We finally found an orthodontist willing to try and bring the canine down. The oral surgeon we used was first concerned after looking at the 3D X-ray that the tooth was laying on the root of the adjacent one but when he went in to place the bracket and chain said it was actually positioned in front of the root. We saw movement after 8 weeks but the following 8 weeks was very minimal. The orthodontist is creating additional space to hopefully get it turning down. Can I send you the X-rays and get your opinion?
Bonjour Madame,
It has been a while since our first conversation. Thank you for coming back. You can send the xray via my professional facebook account: facebook.com/drsylvainchamberland.
It seems that the canine is impacted labially if I read you well.
Hi Karen
I isolate the fields of interest and traced ligns that would help to visualize the movement of the canine.
It is obvious that the canine moved favorably. 8 weeks is a very short period. I usually wait 6 months before taking a new xray.
I would not worry that much for resorption. The canine is palatal, away from the root of the lateral incisors and away from the 1st premolar.
The prognosis is good.
Hello from Spain,
My daugther – 15 years old – has impacted canines with resorption of the roots of all 4 front teeth.
She is in ortodontic treatment for almost 2 years. 8 months ago she got the dental fenestration to pull the canines but it seems that there is no movement al all.
Now they propose to extract the canines and implant
Since the canines are near the roots I am not sure if this will be possible.
I would like to attach some pictures but I do not see the possibility
Thank you for your comments
It is bizarre to find out that the impacted canines is resorbing the roots of the incisors after 16 months or so of treatment. Canine impaction should have been addressed much earlier. WHen they dis fenestration, did they actively pull the canine with an elastomeric chain or a cantilever spring?
It is unlikely that at 15 years, canine can not be bring into the arch.
I would not have the reflex to extract the canine and recommend implants.
You can send the panogram via my professiional facebook page.
My son is 9 and his father got my son’s upper primary canine teeth pulled. I don’t think it was necessary at all. His later inciders were sitting alittle high in the gums but not extreme. I am angry as i was not consulted at all. Can i send a before picture? So you can tell me if i am rightly angry or maybe it was needed.
Thank you
There may be good reason to extract primary canine. You should ask the question to the dentist who did it or orthodontist who recommended it. It seems that there is not a good communication between you and the father of your son. Are you divorced?
You may send me the panogram to my professional Facebook page, but you can call the dentist to get an explanation.
Hi my name is Mandy and I am aged 34 next month. I have just had my 2 impacted canine teeth exposed and bonding when I got out of surgery the surgeon said i have alot of bone surrounding the teeth and that he removed some, also everything I’m reading is telling me that they wont move should i just give up
Chances are good that they will move, but some risk exist that they may not. It is worth to try and you should not regret it. I hope your orthodontist put them on traction.
Hi Amanda
I have the exact same situation as you. I am 41 though. My Ortho said prognosis is good and should move. The surgeon said the same thing about the bone as well. He made a “path” for them to come down. I see my ortho on Monday to tighten up the chains and hopefully pull them down.
Thanks Krista to support Amanda’s decision.
 Thanks for sending your panogram too.
Thanks for sending your panogram too.
The prognosis of the upper left canine is very good. I would it is very easy.
The prognosis of the upper right canine is good too, but it will be more difficult and need some mechanics to achieve final position. The crow is low, I mean near the gingival, not burried thick bone.
I am confiendt that your orthodontist will succeed.
Keep us informed
Would love to hear how it worked out for you. I’m in the same position and wanted to know if its worth going through the surgery or not.
Hi there, I appreciate the wealth of information you have provided on your website.
We recently had a consultation with an orthodontist which terrified my daughter and me. She is 13 years old with had impacted upper canines. During the consultation orthodontist said that impacted canines can cause oral cancer, and can also kill the roots of near by permanent teeth.
This was contrary to a previous orthodontist who two weeks ago said that if left alone the impacted teeth would cause no trouble.
Who can I believe?
What is the prevalence or oral cancer caused by impacted?
First of all, an impacted canine CAN NOT cause oral cancer. Period.
However, some pathology can arise from the dental follicule. The most common would be dentigerous cyst.
In my collection of oral pathology I found this:
1- Dentigerous cyst
This show an elargment of the follicule around the crown of the impacted canine.
2- Central giant cell tumor
Central giant cell tumor is seen predominantly in patients under 20 years of age and occurs more commonly in females than in males, more frequent in the mandible than the maxilla, generally anterior to the 1st molar. This lesion is expansile producing a discernable enlargement and cortex destruction. It may displace adjacent teeth.
3- Odontogenic adenomatoid tumor (AOT)
One can see an enlarge cyst with displaced adjacent teeth involving the lateral incisors and the 2 premolars. The CBCT scan see enlargment of the cortex, displacement of the impacted canine toward the orbit.
Approximately 70% of AOT’s occur in females younger thant 20 years of age and 70% involve the anterior jaw. Association with impacted canine is common. Therefore on radiograph, it can be mistaken for dentigerous cyst.
3-Root resorption
Conclusion
An impacted canine should not be left alone. It may cause significant problems
If a certified orthodontist really mentioned that an impacted canine can cause cancer, I would question where he got that information from because, as far as I know, there is absolutely nothing in the scientific literature to support such a claim…
Thank you for your contribution Dr Lemay.
My 14 yr old daughter has been undergoing treatment for impacted canines. One has descended into place but the other has moved only slightly and is now stuck against and reabsorbing the root of the lateral incisor. I was alarmed by the opinion of the oral surgeon who advised that a root canal on the reabsorbed incisor would have to be done. I declined and insisted on a team consult (the work is being down in a NYC teaching hospital) so for now, some other maneuvers are being attempted by the ortho team to bring the tooth down. Needless to say I am anxious; however I am confused about the long-term health of the reabsorbed lateral incisor. The extent of reabsorption is considered to be minimal. Is is common to offer a root canal for the reabsorbed incisor? Are these teeth at high risk for subsequent problems later?
Sorry for the late reply.
No it is unusual to recommend root canal therapy if the cause of the resorption is the canine that is contacting the root. The direction of pull should be change to move the crown of the canine away from theroot of the incisors.
Once the canine is away and there is no orthodontic force apply on the lateral, there will be healing of surface and the resorption will stop. However, it will never grow again.
I hope the orthodontic team at NYC has solved the problem.
Thank-you for the response
I can report that the oral surgeon reattached the chain at a more distal
Position (I believe) and together with the orthodontist attached more wires to apply strong force to change the direction of the pull.
The force is very strong but I am happy to report that as of last week, the tooth looks to be moving out of the bone and away from the lateral incisor. It has taken approx. 3 months.
We are hopeful 😊
I will keep you informed of the progress but feel disillusioned and frustrated that some orthodontists are willing to write off canine impactions as ankylosis and just quit! I’m also glad that I was firm when the oral Surgeon wanted to do root canals, canine and extraction and an implant.
If you have not done so already, you should publish a case-studies book for professional training. It seems to me that many would benefit from your expertise in this field.
That is good news. Tanks for the suggestion but writing a book is a lot of work. I have difficulty to replys to the many question I received on time. I prefer a website so the information is available for the public, which is the goal. I select the question to provide the most usefull information to the public.
I am also engage in lecturing to graduate student in orthodontics and international orthodontic meeting. I also to run my practice and have a private life.
I am willing to publish the panogram before the 2nd surgery and a follow up that show the teeht has moved if you can get them.
Send it to my professional facebook page.
Best regards
I do understand!
I am thankful to have found your page.
Your insight definitely gave us hope. I will share your site with anyone I meet in future who has need.
Merci beaucoup.
Hi Dr. Chamberland,
Thank you so much for taking the time to give your advice and also for contacting your friend in Ontario. If only we lived in Quebec City, we would definitely work with you. We will get a second opinion here.
Thank you!
Merci Madame
I am sure you will find the answer to your question about your daugther.
If you want to share with us the final treatment plan, it will be much appreciated by me and the internaut in general.
Best regards
Hello Dr. Chamberland,
Thank you for providing such an informative website.
My daughter is 13 years old and she has two impacted upper canine teeth. They are both sitting high above the four front teeth, quite horizontal and in the vestibular position.
Our orthodontist recommends to extract both the impacted and baby canines, and to move all the upper molars forward to close up the space.
We are concerned about losing the canine teeth and also concerned about the risks of the surgery to extract the impacted canines from their position close to the nose area.
The other option is to try to reposition the canines, but our orthodontist says there is a high risk of damaging the roots of the front four teeth.
What do you think would be the best course of action?
Bonsoir,
Chances are that I would recommend the same thing. If the maxillary canines are vestibular and high above the central incisors, likely causing root resorption of the incisors, the safest tx plan might be extraction of the impacted canine and closing the space by protraction the posterior teeth. I hope your daughter has some class II relationship in her malocclusion. This would help. If you look at my answer of February 4, 2017 above, you will see an exemple of one of my case in the 2nd xray. This 1st xray is the case of the internaut.
Do not worry about the position close to the nose, oral surgeon are very good to do surgery without damaging anything.
However, if the canine were palatal, I would likely try to bring them in occlusion.
I hope that help.
Vestibular impacted canine
Merci Mme Marchenko for sending me the xray of your 13 years old daughter.
This confirm the very high position of the canines above the roots of the maxillary incisors. It shows retined deciduous canines, a missing lower left 2nd premolar (#45), retained lower left 2nd primary molar (#75) and a lower lingual arch.
You said that your daughter was followed by your orthodontist since the last 5 years.
One may question why the primary canine were not removed 2-3 years ago and why a panogram was not take when she was 11-12. But it does not give the solution to apply at this moment.
I show the panogram to a friend orthodontist in Ontario. He also ask which orthodontist missed this. However, we both know your orthodontist and we both believe he is a good orthodontist.
About the treatment plan, my friend provide the same alternative.
1- If it is an exo case, we both agree that it would be nice to extract 13, 23, 45 and lower left E (#75)
2- The prognosis of the primary teeth #75 is poor. We should deal with that now.
3- Extraction of upper canine and protraction of the posterior teeth is feasible is miniscrew is used (temporary anchorage device or TADs).
If it is not an extraction case, I would try to bring those canine into the arch. I would not palce braces on the front teeth and would pull the canine with a removable appliance and a cantilever spring. I have done several traction of high canine with this technique without arming the root of the incisors (see mecanotherapy). In the case of your daughter, there is no root resorption. This is an advantage. It is not like the 2 case in the comment of February 4.
I need more information to tell you what I would do or what should be done. I need photos, ceph, clinical exam. There are many good orthodontists in your area. It is your decision if you want to have a second opinion.
Before leaving you, I have a recent case that I took progress panogram yesterday after 10 months of treatment.
Note that the direction of pull is distally and the canine that was horisontal is now vertical and no damage was done to the incisors. I can see the bonded button through the mucosa. The tooth wil be in the moth within the next 2 months.
I hope tthat will help you.
Extraction of 4 premolars is a common treatment plan to resolve sevrer crowding like you describe. You should not worry because your daughter would not be unique to have 4 permanent teeth removed during her orthodontic treatment.
I assume that this recommendation is from a certified orthodontist and not from your general dentist. If not, I strongly recommend that you consult an orthodontist.
My 12 year old daughter’s jaw is too small for a canine to grow. So it is growing on top of her permanent teeth visible in the gums. Our dentist recommended to extract 4 teeth (all permanent) to leave space and have symmetrie – 2 teeth to be extracted left top bottom and 2 teeth right left top bottom. I am really worried of removing 4 permanent teeth. Is there another solution? Thank you
I am 20 years old and I’m live in South Korea. I found impacted canine teeth 18 years old. But my dentist said it couldn’t get right position so I extracted them.
In fact I didn’t know that canine teeth is important.
Now I know canine teeth’s importance, and my premolar teeth get position of canine teeth.
Is it okay if I live without canine teeth? If I live without canine teeth, is there any problem with my another teeth?
And the resorption of central incisors are serious. I can’t send my X-ray but it is really serious. Is it necessary implant surgery of my central incisors? I’m so scary.
Send your xray via my facebook account : facebook.com/drsylvainchamberland
Root resorption of maxillary incisors
Bonjour,
I agree that you have significant root resorption of your incisors and short root of many other teeth, but all your teeth seems correctly aligned and the extraction spaces are closed.
Chances are that at this moment your braces are removed or will be removed very soon. I would use a bonded lingual wire to spint your front teeth together for the retention phase.
I would have done the same treatment plan, ie extraction of the impacted canines and two lower 1st premolar.
I have done a similar case where I had no other choice than to extract the maxillary canines. Root of the central incisors were damaged at baseline and some resorption continue to occur during treatment but with the bonded lingual wire, mobility was reduce and the teeth can be viable for the lifetime.
I hope that help.
Best regards
Hello Dr. Chamberland,
My Son will be 8 years old in 2 days. He has seen the orthodontist who has decided to install an appliance to widen his narrow palate and correct his cross bite. Before doing this, the orthodontist would like to have the 2 baby canines extracted b/c he said the teeth are crowded and the roots look long and twisty and the permanent teeth will protrude in front of or behind the primary ones.
Any input would be greatly appreciated. Thank You (I can send his graphics)
Usually, I do the rapid palatal expansion first. Then I reassess the need of extraction of the primary canines. Keep in mind that it may occur that after expansion, the extraction may not be needed anymore. The reverse is also true, some cases need extraction of the primary canines after expansion.
I hope that help.
i am 19 years old and have a lower impacted canine that has about 12mm to move. hOw long do you estimate it for it to take to get into the right position? Thanks
Mandibular impacted canine
It may take up to 12 months to bring the canine into the dental arch and once it is there, it may take another year to finish its alignment. For more information read impacted mandibular canine both english and french version of the webpage.

See the case I posted on the other page
I am 24 years old.
And both of my front biggest teeth have problem
The right one has a crown but it seems that
Its going to be broken
the other one has has gone they already pulled it and
Im using partial denture for it.
But the x ray show that I do have impacted tooth on both of them.
Will those impacted tooth will still erupt?
Thank you
At 24 years old, the prognosis of foreced eruption of impacted canines is very good. It is sad that you loose your front teeth. I hope that you can find an orthodontist that will recommand you a good treatment.
I am 47 years old and have an impacted upper canine in my palette. I still have a baby tooth in that spot.
My parents were told I should have braces to bring it down but at the time my teeth were straight and they could not afford it.
Now when I go to the dentist there is always concern that the baby tooth will fall out and the space is not condusive for a bridge.
I went to the orthodontist to see about pulling it down but he said it will likely not come down now and could misalign the other teeth.
If the baby tooth falls out an implant can not be put in unless they remove the impacted tooth.
So the surgeon suggested I remove the impacted tooth and hope the baby tooth will stay in.
Then if it eventually it falls out they might be able to do an implant.
Otherwise a denture. Any suggestions?
Even if you are 47 years old, it my be worthed to try orthodontic traction of your impacted canine. Of course the primary canine should be extracted at the same time of the surgicale ligature of the canine. Upon surgical exposition, the oral surgeon will know if the tooth is ankylosed or not and will have a good idea of the prognosis.
You have nothing to loose. If the orthodontist bring the canine into the dental arch, it is a win-win situation. If the canine become ankylosed during treatment, chances are that it will be extracted and a dental implant will be necessary.
I would not count on the primary canine to stay in your mouth for long term.
Of course, my comments are done without having seen the panoramic radiograph of your impacted canine. This would have help for recommendation.
I am 65. I remember being told about my unerrupted canine 40 years ago but until this year i had totally forgotten. Then the tooth began to errupt .
So this morning I have had it extracted.
My teeth in my top jaw are almost all crowns.
Will I have problems with them?
Thank you
It is sad that during all those years you had several dental treatment to place crowns on your teeth and nobody reminded you that you had an impacted canine that should have been bring into occlusion.
The problems you may have with your corwned teeth will liklely not be related to the removal of your impacted canine. However, some dental movements may occur.
I am 51 years old. I started orthodontic treatment eleven years ago to move the impacted canine in position. It has finally come in place in all its glory. Within a two month period it made a significant move. What are some of the implications that I need to consider after all these years of treatment?
Eleven years of orthodontic treatment? Wow!
I would consider if there was root resorption that might have occureed and possible bone loss around the erupted canine.
I would recommend retention protocal that may include a removable appliance or a retention wire bonded to the lingual of your 6 anterior teeth.
I’m 21 years old, and was told at 13 my front right canine would never grow in. They left it, and at 18, it pushed past my other teeth and turned itself sideways. At 21, it’s only halfway grown in, and is constantly swelling. Could it be infected? Does it need to be pulled? I’m not sure what to do. Thank you.
You should consult an orthodontist or at leat visit a dentist. I do not recommend extraction of the canine. You may have periodontal abcess if the tooth is partially erupted.
Visit a dentist or an orthodontist.
I would not hesitate in this situation to extract both primary canine (53 and 63) and because he is 13 years old, i would also extract both primary first molar (54, 64).
Please note that the permanent upper right canine (13) is likely located palatally because we can see the superimpostion of the root of the lateral incisor over the crown of the permanent canine.
If they don nothing, like not extracting the upper left primary canine, they increased the risk of impaction.
Self eruption of a high canine
The picture above show the effect of the extraction of a primary canine on an impacted permanent canine. You can see that the follow-up radiograph depict self eruption of the permanent canine over a total of 29 months.
Of course, the upper left canine of your son is higher and more horizontal, the pronostic of self eruption is not has good, but it will likely move in a more favourable position if the primary canine and 1st primary molars are extracted.
In conclusion, i would extract teeth 53, 54, 63, 64 and reassess in 6 and 12 months. I would tell you that surgical exposition and ligature will likely be initiated in 12 months or so.
I hope that help.
.
Thank you for your reply.
My son will turn 13 in a couple of weeks. I’ve been told he has an underdeveloped mouth for his age-more like that of a 10 year old. He still has many baby teeth.
They want to leave the baby canine below the impacted one in case they remove the permanent one later, remove the baby canine from the other side, and remove the tooth behind the canine on both sides.
They then want to do nothing and wait a year to see if the impacted canine moves at all on it’s own. I worry about another year going by and not attempting to aid the movement of the canine. I’m afraid if the root grows more, it will anchor in and not be able to turn.
Is there a way I can send his X-ray for you to see?
Under impaction and ectopic eruption, you have an X-ray of a horizontal permanent canine labeled 2. Were you successful in getting this tooth in position and erupting?
My son’s X-ray has one canine in that same position and they are saying it can’t be moved and needs to be permanently removed.
This worries me since the permanent canine is an important tooth.
I don’t want to remove it unless I’m positive it can’t get into position.
Yes,I was successful bringing this high canine into occlusion. The case is presented in the keynotes Treatment and management of impacted canine with SPEED appliance slide 40 to 56.
This patient was 13-14 but I have treated patients in their early 20s with same success. The older they are, the longer it takes.
You are right that canines are important teeth and even if I elected to recommend extraction of some impacted canine, it is rare.
This is the exemple of a 17 years old man when I begun his treatment. The progress panogram is after 3 ½ years of treatment. It is 3 years longer than the 14 years old boy. But I got it done. I will finish by Christmas.
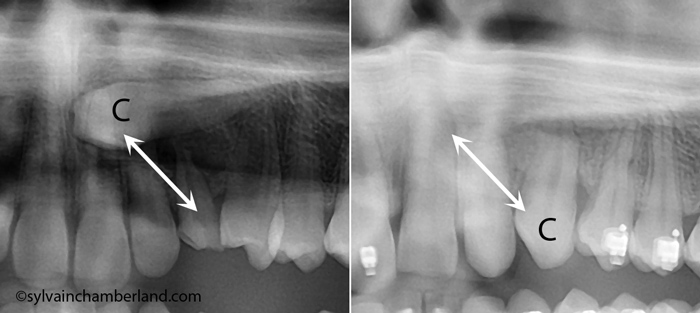
Please help,my son is 13 years old soon to be 14 he has an impacted tooth covered by bone #11 ,he was all set for the surgery and the week before his surgery the surgeon calls and now wants a second opinion,I this a risky procedure and what can Happen if he doesn’t get it done ,also my son has Tourette tics ,he is in no pain from this tooth however he does have braces and the orthodontist wants to put a prosthetic tooth in the #11 place ,what do I do
If the surgeon asked a second opinion because the 1st orthodontist wanted to extract the canine, I totally agree with him. The orthodontist should bring the tooth into the arch unless it is proove to be impossible to do it.
I would not extract a permanent canine in a 14 years old children to place an implant even if this patient have Tourette syndrome. I have treated some patient with this syndrome and they are not difficult to treat. I treat patient that have autism also.
I hope taht help.
Best regards
Thank you for explaining these issues in such a way that anyone could understand. Hats of to you.
Sylvain
As always a great job on these issues of concern to the public and the profession.
Keep up the good work.
TDC