The comments
Dr. David Briss says:
It was my pleasure to meet with Cary and go over his case.In my note I left out our discussion of the disc displacement; I did find anteromedial disc displacement with reduction, but with no limitation in any excursive movements, no history of pain or locking.
He did indicate to me that he has intermittent right ear pain, perhaps this is related to the more narrow nasal cavity on the right side, possibly some blockage resulting in intermittent middle ear inflammation.
Given the appearance of the condyles and the lack of a functional shift I doubt that the ear symptoms are related to the joint sounds.
Dr Sylvain Chamberland, Orthodontiste says:
Thank you Dr. Briss for this thorough report. You were my eyes at far distance.Your tentative treatment plan is close to one of my hypotheses: extraction of 3 premolars and a sliding genioplasty. It is unfortunate that I missed the posterior right crossbite, but I could not see this from the reconstruction xray.
We went as far as we could get with an internet consultation.
I wish you all the best.
Dr David Briss says:
I met Cary at my office yesterday, and on clinical exam he is Class II div 1 subdivision right malocclusion, maxillary midline deviated approximately 1mm left and mandibular midline deviated approximately 3mm right.There is slight bimaxillary crowding and an overbite of approximately 3mm. He has the remnant of a crossbite on the right side (1.6 and 4.6 are end-on transversely). Significant dental history is a PFM crown on 2.1, and he had orthodontics as a child, but no palate expansion was done. His chief complaint is facial asymmetry, particularly mandibular asymmetry and chin deviation.
The radiographic reconstructions he provided me seem to show the condyles positioned relatively well in the fossae. The cortex is intact, there is virtually no evidence of flattening of either condyle. There does not seem to be any evidence of pathology.
The panoramic reconstruction appears to show a deviation of the nasal septum to the right, but this is not obvious on the PA cephalogram reconstruction. In PA he does have a significant sloping of the floor of the nasal cavity, higher on the right than the left. The J points do not appear to be as asymmetric as the nasal floor finding might indicate. On facial examination his right orbit is noticeably higher than his left orbit. The chin is deviated to the right of the facial midline.
I suspect the etiology of his malocclusion and asymmetry is related to maxillary constriction, possibly a crossbite and mandibular functional shift that was never skeletally corrected during his prior orthodontic treatment.
In the absence of a current posterior or anterior open bite, and with images of well defined condyles I do not feel that there is either condylar hyperplasia on the left nor resorption on the right. It probably warrants followup at some time in the future, but at the moment it does not appear to be a progressive problem.
The only orthodontic treatment option that might satisfy his chief complaint would be combined orthodontics/orthognathic surgery. This most likely would be SARPE followed by limited orthodontics, then a Le Fort 1 for rotation of the maxilla (to the right) and asymmetrical BSSO with rotation to the left. However, this amount of treatment may result in only a small gain in aesthetics compared to a sliding genioplasty, and I would not recommend surgical orthodontics at this time. Additionally, an orthodontic-only treatment plan would perhaps correct the malocclusion to Class I bilaterally, but with no affect on the facial aesthetics, and is therefore not indicated either.
Dr David Briss
Orthodontist
5 Village Square
Chelmsford, MA 01824
Dr Sylvain Chamberland, Orthodontiste says:
Do you give the permission to publish a short report of your consultation with Dr David Briss?Dr Sylvain Chamberland, Orthodontiste says:
Hi Cary, I have been informed that you visited Dr. David Briss. How was the consultation with him?Cary says:
Yes, you have my permission to publish anything related to my case. I only ask that sensitive information or anything among those lines be covered.Looking forward to seeing the story!
Cary says:
And thanks again for all your help. Dr. Briss was great! Truly insightful. In the end, he felt my case wasn’t severe enough to really consider jaw surgery, which I was actually happy to hear.Dr Sylvain Chamberland, Orthodontiste says:
Your MRI report says there is no evidence of a disk dislocation which is good news. I would not worry that much about the other findings since you have no pain and no limitation of jaw opening.It is difficult to assess condylar length with the pict I received. The panoramic view is reconstructed from 3D. No doubt there some left condylar hyperplasia that has occurred. The important thing to assess is if it is still growing or it is in remission.
I would like to remind you that the information I gave to you is a hypothesis. It is not intended to be a thorough diagnosis nor any suggestion I made would be considered final treatment plan.
I don't think I can help you further than I did. I saw that you come from Boston. I would recommend you my good friend Dr. David Briss. He practises in Boston and teaches at Boston University.
Cary says:
Thank you Doctor, I will try to get a bone scan as soon as possible and let you know. Based on the initial CT images though, do you see any evidence of condylar hyperplasia?I just got my MRI report back which my oral surgeon said the findings were “insignificant” but I thought I would share with you anyway since to me, the results seemed quite the opposite. Perhaps you know a better oral surgeon in the Boston area?
Any input would be greatly appreciated.
Thanks.
Dr Sylvain Chamberland, Orthodontiste says:
 Regards to extraction, I said premolars which are about 7,5 mm wide, not molars that are 10-12 mm wide. I said only one premolar in the lower left quadrant which will allow midline correction, but minimal lower incisors retraction if there is some crowding, a little bit more retraction if there is no crowding. The less the lower incisors are retracted, the less the effect on lip support. Nevertheless, we are talking about 1-2 mm of lip retraction.
Regards to extraction, I said premolars which are about 7,5 mm wide, not molars that are 10-12 mm wide. I said only one premolar in the lower left quadrant which will allow midline correction, but minimal lower incisors retraction if there is some crowding, a little bit more retraction if there is no crowding. The less the lower incisors are retracted, the less the effect on lip support. Nevertheless, we are talking about 1-2 mm of lip retraction.Regards to surgery, you may benefit from orthognathic surgery if you want to have a straighter profile or correct the vertical asymmetry in the frontal plane.
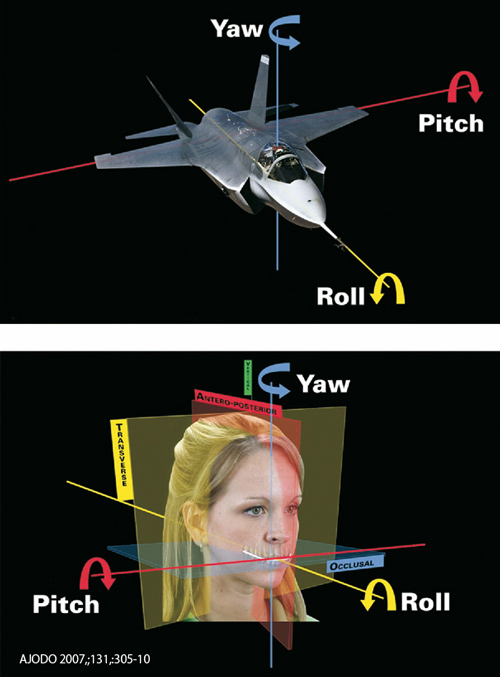
I am not sure you would need counterclockwise rotation of the occlusal plane (decrease pitch) because the 3D and ceph view shows a fairly normal angulation of the occlusal plane to the Frankfort plane (FH).
My concern is that you don't have an increase overjet, therefore, there is no room to advance the mandible. Extraction would be necessary to create an overjet that would allow mandibular advancement. If so, extraction of 1 lower left premolar may be what is needed (non-extraction in the maxillary arch).
Your facial asymmetry, if one wants to correct it, need "yaw" correction of the mandible and "roll" correction of both maxilla and mandible.
 I did not have the profile view that would include your ear and your eye to correct and position it in the true horizontal relationship. With this profile view corrected to the plane "subnasale vertical" your mandible doesn't look that much retrusive.
I did not have the profile view that would include your ear and your eye to correct and position it in the true horizontal relationship. With this profile view corrected to the plane "subnasale vertical" your mandible doesn't look that much retrusive.Finally, I would like to clarify that if you elect to do an ortho treatment with or without surgery, the joint clicking may still remain. Orthodontic treatment of orthognatic surgery don't cure TMJ derangement.
The MRI will tell something about the disk relationship in the glenoid fossae. It does not say anything about growth activity. To assess growth activity, you need to have a bone scan (scintigraphy with Tc99).
Cary says:
Thank you so much Dr. Chamberland for your detailed reply. Would you mind looking over a few follow up questions I have?– First off, for my case, would you not recommend considering jaw surgery? I was told previously by one oral surgeon that despite the fact my jaw is only slightly recessed, I would still benefit from CCW rotation and correction of the midline deivation which could only result from jaw surgery.
– Also, with regards to molar extraction, would this not cause the mandible to recess even further back?
– Finally, in your opinion, do you believe my facial asymmetry (not just jaw, but eyes, and ears as well) could be the result in the differing sizes of my condyles? Or, do you believe my facial asymmetry was simply more skeletal growth related?
I actually just had an MRI yesterday, so I hope they can tell from that whether the condyle is still growing or not.
Merci, Doctor.
Dr Sylvain Chamberland, Orthodontiste says:
Merci Dr VenditelliDr. Bruno Vendittelli says:
Bravo! What a fabulous article.Eugene says:
Thank you very much for your answer. Probably, it will be removed. I do not know how, it will be decided today.Dr Sylvain Chamberland, Orthodontiste says:
How do you assess that the upper jaw is not sufficiently forward?If you have 2 mm normal overjet and 2 mm normal overbite, chances are that the upper jaw is properly place over and in front of the lower jaw.
However, if you feel that you malar bone (cheekbone) are flat despite maxillary advancement, this may be explain by the fact that you had a very deficient maxilla and you might need cheekbone implants.
On the other hand, if you had a retrognathic maxilla that need maxillary advancement, it is very unsual to bring the mandible forward at the same time. This make no sense.
I would like that you specify what type of movement you really had and why.
Dr Sylvain Chamberland, Orthodontiste says:
Eleven years of orthodontic treatment? Wow!I would consider if there was root resorption that might have occureed and possible bone loss around the erupted canine.
I would recommend retention protocal that may include a removable appliance or a retention wire bonded to the lingual of your 6 anterior teeth.
Dr Sylvain Chamberland, Orthodontiste says:
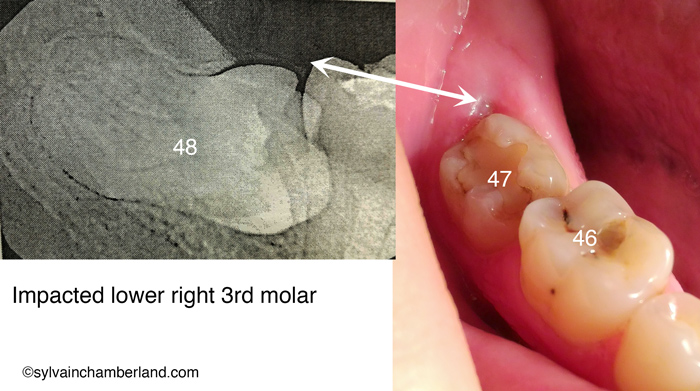
Hi Eugeny,I would defenitely recommend the removal of the wisdom tooth. The white double end arrow indicate it is partially erupted. You can see 2 -3 mm of the tooth in the right picture that match with the xray on the left picture. This partially erpted tooth is at high risk of infection (periconitis) or causing decay or resorption of the root of the 2nd molar (#47).
However, the tooth may be at risk of causing nerve damage if the dental surgeon is not experimented. In Quebec, the removal of this tooth by an oral surgeon would not be a problem.
I hope that help.
Evgeniy says:
Hello.I do not speak in English (writing via Google Translate).
I read your article on wisdom teet.
And I realized that you're a real expert!
I live in Russia. The level of medicine we have a very poorly developed. It is very difficult to get professional help even for money. I wanted to ask you whether the Council should remove my wisdom teeth. I am 29 years old. I enclose a photo and X-ray of the tooth. It tried to make a good photo. Hopefully we will see. In the photo you can see a bit of what became erupt gums. The tooth does not disturb. Only the unpleasant smell of the place. Do you think whether it is necessary to remove the tooth. Or, you can not delete. The root of the tooth may touch a nerve - found out about this from your article. I'm afraid I will trust in our doctors. They can easily pull out a tooth without understanding. Please help advice.
Here is a photo:
Please tell me whether you can see on the x-ray shot that touches the nerve of the tooth? If the tooth should be removed, it is necessary to complete removal or partial removal of a tooth?
Sincerely, Eugene.
Ana says:
Greetings,I am 28 and I had double jaw surgery.moving the upper and lower jaw forward.
I am not satisfied because the upper jaw is not sufficiently forward.
Can you fix this and move the upper jaw forward without surgery?
How much? The length of time required?