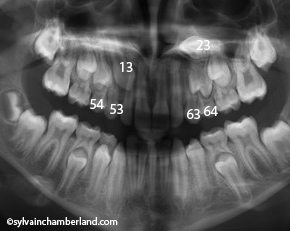
It is a big mistake to maintain the upper left primary canine (63) and planning to remove the permanent canine later (23).
I would not hesitate in this situation to extract both primary canine (53 and 63) and because he is 13 years old, i would also extract both primary first molar (54, 64).
Please note that the permanent upper right canine (13) is likely located palatally because we can see the superimpostion of the root of the lateral incisor over the crown of the permanent canine.
If they don nothing, like not extracting the upper left primary canine, they increased the risk of impaction.
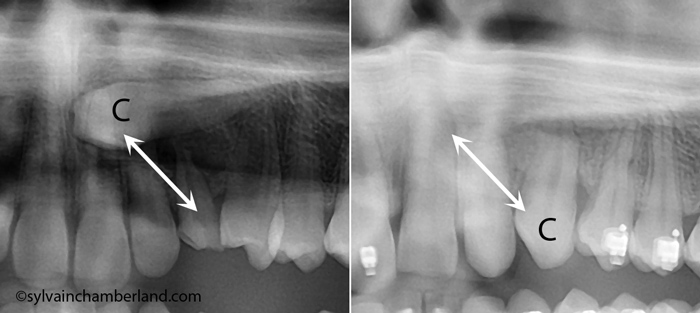
Self eruption of a high canine

The picture above show the effect of the extraction of a primary canine on an impacted permanent canine. You can see that the follow-up radiograph depict self eruption of the permanent canine over a total of 29 months.
Of course, the upper left canine of your son is higher and more horizontal, the pronostic of self eruption is not has good, but it will likely move in a more favourable position if the primary canine and 1
st primary molars are extracted.
In conclusion, i would extract teeth 53, 54, 63, 64 and reassess in 6 and 12 months. I would tell you that surgical exposition and ligature will likely be initiated in 12 months or so.
I hope that help.
.
 Thank you for sending me the xray of the impacted canine of your 15 years old son.
Thank you for sending me the xray of the impacted canine of your 15 years old son.